This Summer in M’Finda Kalunga Garden Intrepid Volunteers Kepy the Garden Open
Working and welcoming and Keeping Safe Practices. Thank you volunteers!


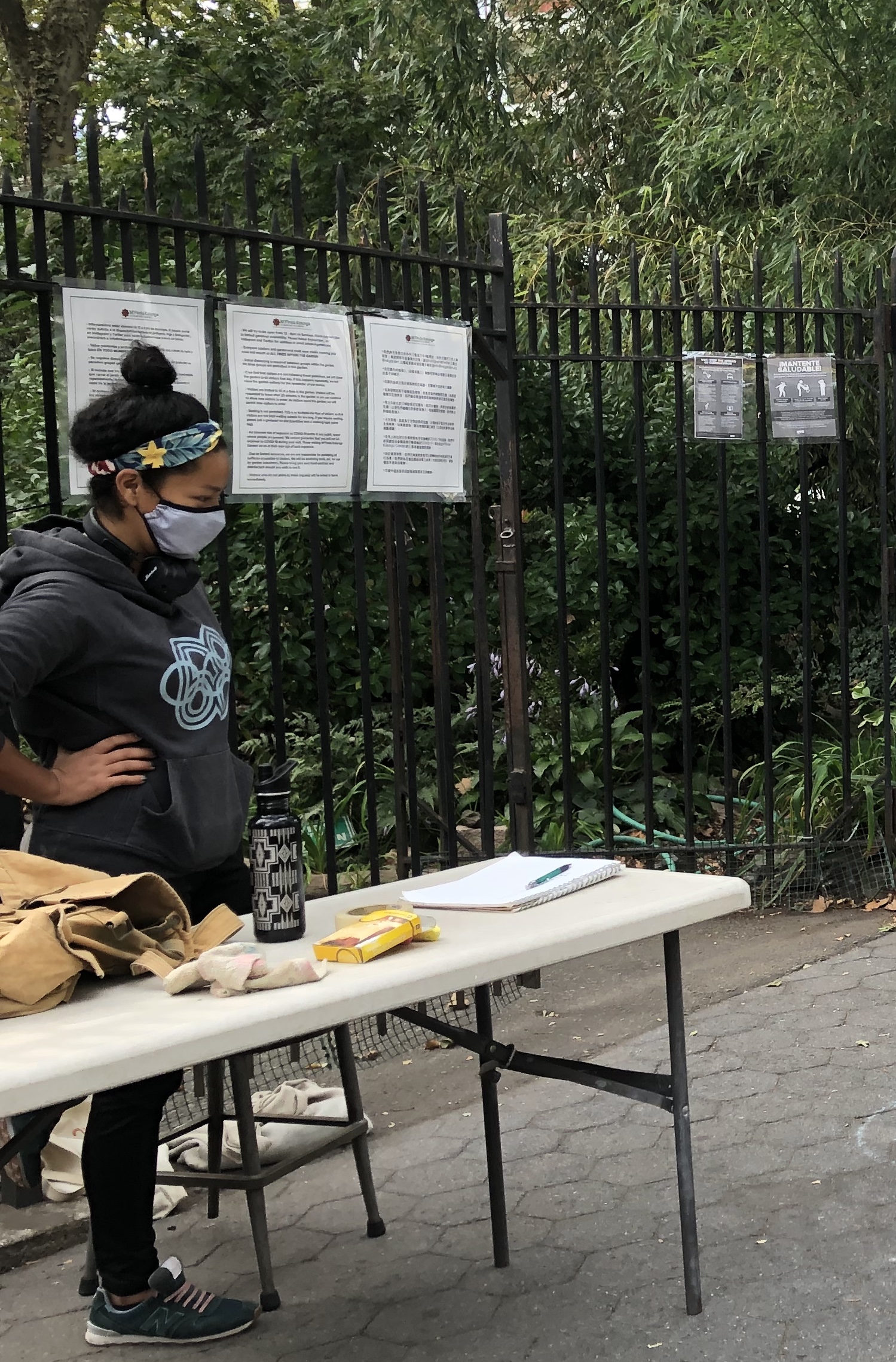

Working and welcoming and Keeping Safe Practices. Thank you volunteers!
A GREEN PUBLIC WORKS PROGRAM FOR NYC: 40 IDEAS FROM EXPERTS
Full plan here
A Green Public Works Program for NYC: 40 Ideas from Experts To understand how New York might take advantage of federal investment to create jobs and help the city mitigate and adapt to the effects of climate change, CUF asked city leaders in coastal resilience, environmental justice, urban agriculture, renewable energy, and more for sustainability and resiliency project ideas. by Laird Gallagher, Safiyyah Edwards, Cameron Haas, and Jonathan Bowles

Some of the ideas include:
Jeffrey Raven
Principal
RAVEN A+U
Build a network of energy hubs
The city should build neighborhood energy hubs to store energy in large-capacity smart grid batteries, and secondarily act as recharge stations, bike storage, drop-off centers, civic spaces, or last-mile freight hubs. Placing energy hubs throughout New York City’s neighborhoods would not only build energy resiliency within communities but act as colorful and aesthetically important symbols of each neighborhood. These colorful iconographic structures would be designed to reflect New York City’s neighborhood identities and needs, instantly becoming 21st century icons on the urban landscape.
Pat Sapinsley
Managing Director of Cleantech Initiatives
Urban Future Lab, NYU Tandon
Repurpose public land into renewable power plants, microgrids, and energy storage
Replacing fossil fuel-based power plants with renewable energy plus long duration energy storage facilities has been shown to result in significant cost savings in healthcare as well as job opportunities for the surrounding communities. Rikers Island is especially well-suited for this conversion, and has growing support as evidenced in the Renewable Rikers Act.
Clare Miflin
Founder
Center for Zero Waste Design
Develop neighborhood-scale composting infrastructure
Equipment in large buildings can reduce odors, pests and the volume of organic waste by up to 90 percent, making it easier for understaffed and space-constrained buildings to manage. Investments in local composting infrastructure can increase processing capacities greatly, and excess organic material could be returned to the regional farm system.
Hildegaard Link
Chair, Resilient Red Hook
Director, Sustainability, SEBS Rutgers University
Build energy resilience through community solar
Neighborhoods served by above ground power lines are especially vulnerable to extreme weather. Constructing a microgrid powered by community solar would allow the neighborhood to power residents, businesses, and essential public services during emergencies that often plague the low-lying, coastal communities like Red Hook. Constructing a community grid of solar energy sources would also work to unify neighborhoods. A community solar grid could help to foster a shared sense of ownership within the neighborhood and also respond to the unique needs of local small businesses.
Hana Kassem
Principal
Kohn Pedersen Fox
Revise East Side Coastal Resiliency Plan to leave park intact
The current East River resiliency proposal calls for raising the majority of the park above the 100-year flood plain, but that requires cutting down many of its trees and the phased decommissioning of large portions of the park. But given how vital the park is to multiple neighborhoods for exercise, social gathering, and informal cultural activities, especially during Covid-19, it may be worth revisiting the earlier version of the plan, which left most of the park intact by creating a flood barrier wall with flood gates along the east side of FDR. This resiliency strategy could be taken up again for the majority of the park, thus saving the park trees and maintaining its accessibility in some form during construction.
Reconfigure flood protections under FDR Drive to provide new, Covid-safe uses
What if we rethought the underbelly of the elevated sections of the FDR to become a series of raised outdoor covered rooms that allowed for a variety of safe uses? These raised platforms would be combined with barrier walls and flood gates, positioned astutely to provide the necessary flood protection. To extend their use into the colder months, these outdoor rooms could be outfitted with solar-powered outdoor heaters and lighting. This large-scale project would foster social interaction and community spaces, boost the local restaurant and retail industries, reignite the city’s cultural life, promote health and wellbeing, all while addressing resiliency, sustainability, wellness and creating jobs.
Justin Green
Founder and Executive Director
Big Reuse
Construct reuse centers in every neighborhood
Material reuse can both help the environment and create local economic growth. Instead of buying a dresser that was made in another country from recently cutdown trees and shipped around the world—we can reuse locally. In addition to the initial labor needed to build reuse centers, these facilities can create jobs for workers to manage and operate the facilities. Reuse and repair centers not only keep materials circulating within the community; they also keep the money exchanged for goods, repairs and refurbishment within the local economy, too. In the long term, these centers also encourage sustainable shopping behaviors. Reuse centers can create jobs, keep materials out of the landfill and become close to self-funded with some additional support for transitional workforces.
Repurpose portions of public space & parkland into community composting sites
Constructing composting sites would generate jobs not only from site development but from running the pickup and composting programs. This will encourage local composting and generate compost to divert materials from waste streams going to landfills.
Paul Gallay
President and Hudson Riverkeeper
Riverkeeper
Invest in community-driven, nature-based coastal resilience projects
With sea levels rising, New York City must support community-driven, nature-based solutions for coastal resilience. Rather than focusing on expensive offshore storm surge barriers, the city should construct onshore environmental infrastructure such as berms, living shorelines, salt marshes, and wetlands which provide cheaper, more adaptable, and less ecologically destructive protection against sea level rise. Projects such as stormwater retention gardens and salt marsh restorations have already been successfully completed in other northeastern cities like Boston. Native plants and trees that can survive both dry and flooded conditions should also be prioritized in coastal communities. A workforce tasked with plant stewardship can be responsible for the long term care of these plantings. In designing and executing these climate-smart projects, front-line communities should be central, especially historically disempowered and BIPOC communities.
Candace Damon
Vice Chairman
HR&A Advisors
Support maintenance projects
The default progressive response to economic downturn is to invest in capital projects that can be advanced quickly and that address other contemporary policy priorities—today, resilience, climate adaptation, and equity. Virtually by definition, however, shovel-ready capital projects are those which have already been funded; directing stimulus funds to them replaces one source of funds with another. While New York City should certainly welcome any expansion of its investment capabilities, the shovel-ready projects for which there is no other source of funding, indeed for which there is vastly diminished funding, are maintenance projects.
I would prioritize restoration of parks—despite being, as always, the first operating budgets cut, parks have once again demonstrated their value as critical infrastructure—and clean and efficient energy projects, including weatherization of homes and tune-up of building systems. But we should also support repair of major infrastructure, operating subsidies to strengthen regional food distribution and launch local agriculture, and a host of other maintenance projects that can be initiated within weeks of funding. These projects will all renew the aims of the Civilian Conservation Corps, this time ensuring that women and Black men get equitable access to jobs that are both less likely to be automated in the near term and offer career ladders.
Thanks to neighbors Jeffrey and Tessa here are photos removing the Belgian Blocks. The MTA Contractor Cruz promises these will return after the dig. Parks Department workers also say there are plenty of these stored for Park use.



and information on the coming dig on Forsyth Street.
And complaints about Park vehicles taking up space in the water sprinkler area of the Stanton Parkhouse area of the park since it was fenced off to keep drug dealing and use for storage by homeless or in shelter New Yorkers.
Apparently they have been removed along with the fencing.


From the Educational Alliance:
An American Kestral was caught on camera by Colleen Corkery neighbor and M’Finda Kalunga volunteer.
Katie Leung from the WildLife Unit of the Parks Department ”
“…these feature an American kestrel. I think you’re also lucky to see a kestrel with its meal in talon!”
Colleen wrote, ”
Here are pics…when it was on the lookout..with its catch and snack: a finch!”
Thank you to Bud Shalala MK Garden’s Critter Committee founder for letting us know about the photos!






Ted and Jose get the turtles ready for their winter vacation home.


From the Stanton Task Force:
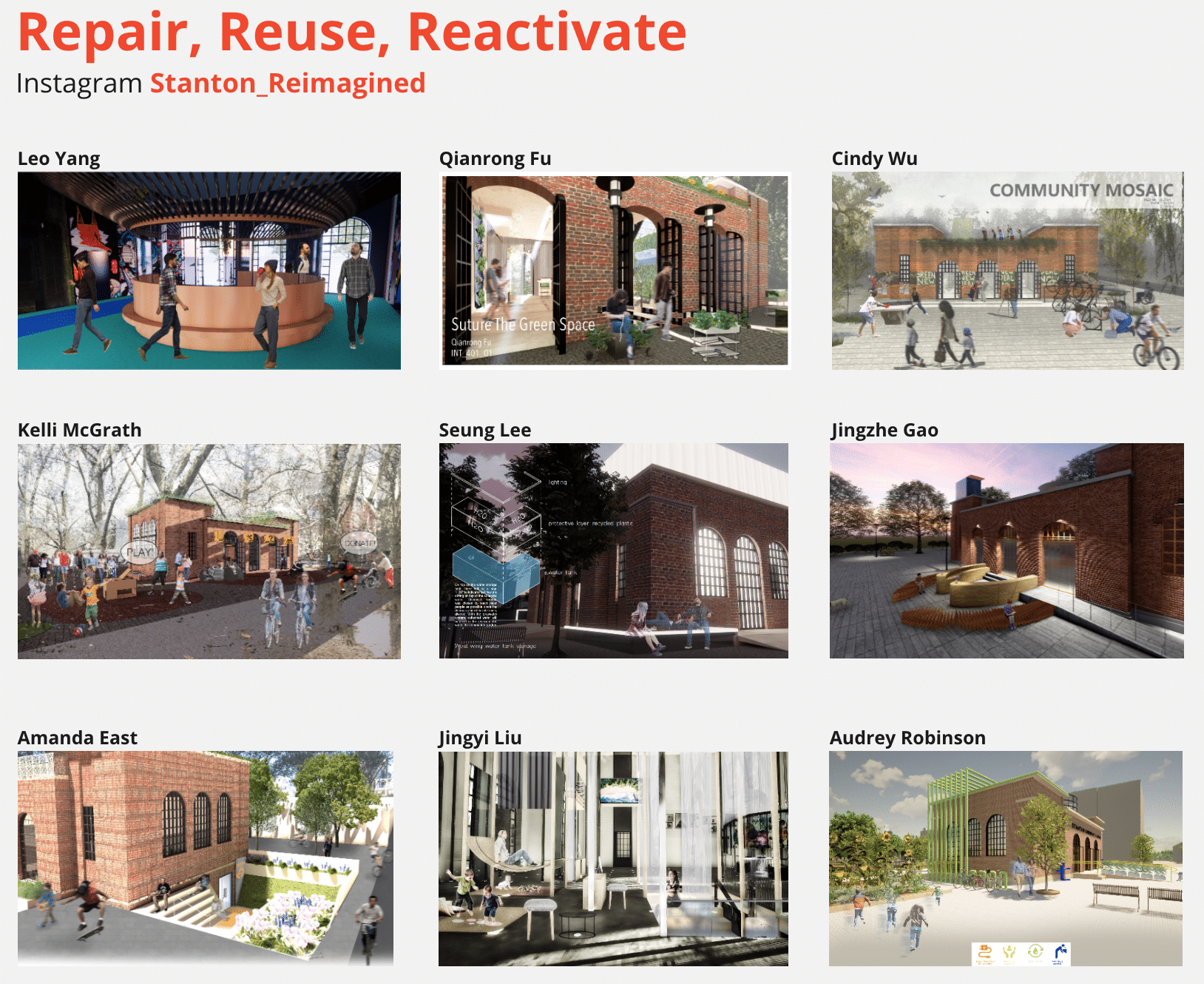
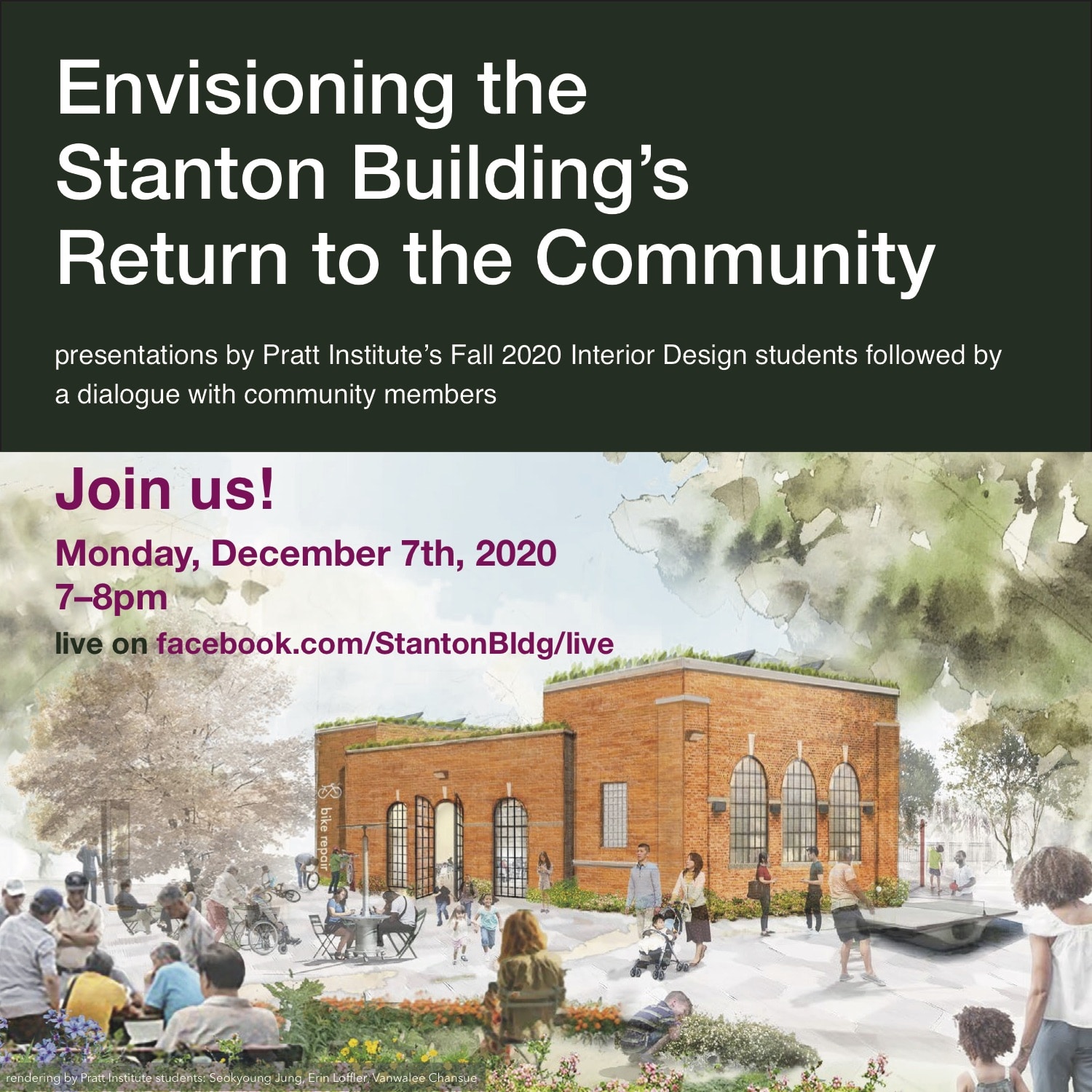
Students from the Interior Design program at Pratt Institute offered their fresh thinking and design skills to our community vision for the Stanton Building in SDR Park.
Brief presentations by these Fall 2020 students of their designs for the Stanton Building were followed by a dialogue with community members. For more detailed views of their work: Stanton Task Force Facebook Page: https://www.facebook.com/StantonBldg/
To Stanton Street Pratt Students: We thank you for showing up in this time of hardships around the world. Our neighborhood, our representatives, Pratt professor Keena Suh and all of you in her classes continue to show us what it means to be a community that is not bounded by self-interest or ‘ownership’ or state or country but bound together with shared work and caring and our future.
“What matters is the countless small deeds of unknown people who lay the basis for the significant events that enter history. They’re the ones who have done things in the past they’re the ones who will have to do it in the future.” Howard Zinn
We live on Lanape land and give our thanks.
‘If you’ve come here to help me, you’re wasting your time. But if you have come here because your liberation is bound up with mine, then let us work together.’ -Lilla Watson, Australian Aboriginal Elder
Parks needs volunteers like never before. And they need a budget to ensure a steady effort to keep parks, clean, functional, bird and plant habitats and safe – integrating model climate mitigation efforts, recreation, play, quiet contemplation, walks, sports, gardening, community gathering, bird watching, habitat restoration, and more.
“Even as pandemic-induced restrictions have lifted, neighborhood parks have allowed life to unfold in ways that still aren’t feasible in cramped apartments. They’ve always served as communal backyards, but now they’re the best gym in town, host get-togethers that would’ve happened in bars and reception halls, and serve as a respite for those working from home or the unemployed. …”
New Yorkers Step in to Keep City Parks From Turning Into ‘Junkyards’
“Because of the pandemic, the parks system cut $84 million from its budget, which paid for 1,700 seasonal workers that typically care for our parks each summer…”
“…the budget cuts have forced a maintenance hierarchy for city parks, with playgrounds and barbecue spots at the top…Up to 500 Parks Department sites might go an entire week without a visit from a parks worker, making volunteers the last line of defense for spaces like Pelham Parkway.”
“…But without city funds, our parks could permanently deteriorate at a time when they’ve proved essential. “Volunteers don’t replace staff — they just don’t,” said Heather Lubov, executive director of the City Parks Foundation.”




























From the Wildlife Unit of NYC Parks:

“…the next season of raptor nest monitoring and scouting is almost here. If you would like to join us for the 2021 season, please let us know with a reply and r
eturn the attached waiver signed, either scanned or photographed.
As a note, great-horned owls and bald eagles may currently be in their courting phase. Keep an eye out for them until we provide you with further details, including the online training webinar.”
We look forward to hearing back from you.
Cheers,
Katie Leung (she/her)
Associate Wildlife Biologist®
Field Technician
C 646.832.6534
NYC Parks
Wildlife Unit
1234 Fifth Avenue, 5th Floor
New York, NY 10029
Thank you Joseph and Davis Fox for removing ice and snow on the paths in the M’Finda Garden!
And for moving donated supplies to weather proof areas.
And thank you to the Boy Scouts and Scoutmaster Troop 150 for advocating for young people to help out.
It will make getting to through the garden for our year round gardeners far safer!
